Door to MD / Door to Mid-level Treatment Time Simple Sampler
Statistics Shmatistics!
Got a watch? Can you count to ten? Like INSTANT results?
Want your Emergency Care Door-to-MD / Mid-level Treatment time down to BELOW 30 minutes RELIABLY, or your Urgent Care Door-to-MD/ Mid-level Treatment under 15 minutes?
Why measure it and "wait for the data" when you can
SEE IT!
TRACK IT!
and F I X I T !
at THE SAME TIME?
Such a deal!
POSTED EMERGENCY ROOM WAITING TIMES ARE OFTEN FAKE
We have seen a recent trend in Emergency Services and that is posting waiting times on billboards, or the Hospital's internet front page that are very short - 20 minutes, 15 minutes, 10 minutes.
When we dig into the data, we find that the traditional standard measure of Door to Treatment (that includes Patient entrance into the waiting area, greeting, registration, triage [in Waiting Area or at bedside], Caregiver Assessment/Teaching, initial lab draws, MD / Mid-level reviews chart and then MD / Mid-level enters room, assesses and begins Treatment) is not actually being used. A new measure has been created. The traditional measure was called Door to MD / Mid-Level Treatment.
And the new measure is called "Waiting Time to Being Seen": But not necessarily seen by the MD or Mid-Level. Sometimes it is "waiting time to be seen" by a greeter or clerk. When it is an MD, Mid-Level or RN, it is not necessarily "waiting time to be seen" for actual Triage and Clinical Assessment; often it is nothing more than "being seen" by an RN, Mid-Level or MD passing through the waiting area, or initially greeting the patient at the front desk. No actual history, assessment or anything that could legitimately qualify as clinical work is being done at that point where this "waiting time" is proclaimed as over.
The actual formal clinical Triage assessment is still later in the process. And the additional waiting time to get there is now hidden from the claimed metric for "waiting time".
Furthermore the "waiting to be seen" metric doesn't always begin at the door. Originally, the "Door to MD / Mid-Level Treatment Begins" started when the patient first entered the door of the waiting area or the Emergency Trauma entrance of the Hospital.
The new metric doesn't start at the door. Now the starting point for this time measurement begins when the Registrar enters the patient's information into the computer, and that is generally when the patient is registered.
That happens after the patient has walked in the door, and after they have waited often at the end of a long line to speak to the registrar. Or simply waited for some time until a registrar or RN returned to the waiting area desk. Is this really the fair starting point for the patient's experience? No. The starting point is the moment they open the door and walk in or are rolled in.
A great deal of actual waiting time has been hidden from this highly touted new statistic, making it misleading.
But it makes the waiting time to RN, MD or Mid-level, indeed the entire Emergency Deparment Length of Stay look much better than it actually is!
Yes, metrics can be faked and often are.
These are all part of cutting corners on the metric to make the numbers look better because they are not actually part of making the flow more efficient for patients.
These times are not Door-to-MD / Mid-Level Treatment times according to the standardized, traditional metric.
DIRECT-TO-BED DONE WRONG MAKES THINGS WORSE
Some hospitals do bring patients directly to the bed in back when there is an empty and staffed bed, and this is a great strategy to reducing waiting time and potential medical error. But only so long as the RN completes the Triage work, initial labs, assessments and immediate interventions that are all part of the appropriate clinical pathway IMMEDIATELY when the patient is brought back. This expedites the MD /Mid-Level entering the room sooner to make their full assessment and begin formal intervention.
But Direct-to-Bed alone is not a fix and in isolation can make things worse, adding delay, neglect and medical error because, as we have seen, this can be used to warehouse a patient in the back where they are now isolated and still don't get rapid treatment.
Indeed, in some cases delays got longer, and clinical issues arose from those delays because the waiting room looked empty; the patient was now "out of sight - out of mind"; and no one really knew that the patient waiting in an Emergency Room bed in back hadn't yet been seen by RN, MD or Mid-level.
In fact, once they were placed into a bed in back, their actual status became a mystery - they fell into a crack in the process that looked on the tracking board like they were being assessed and treated, as though they had been seen by the RN but "seen" and "treated" are two different things - so the patient fell into a void, a twilight zone. On the tracking board, they were in a bed with an assigned nurse, maybe even seen by her or him so it looked like something was going on. But the RN assigned to that bed had not actually taken the assignment of that patient.
This is the problem with popular solutions that are not made in concert with actually changing the responsibilities, competencies, teamwork and communication points, but merely fixing the physical flow, or mechanically and mindlessly tracking data points in the computer.
The actual formal clinical Triage assessment is still later in the process. And the additional waiting time to get there is now hidden from the claimed metric for "waiting time".
Furthermore the "waiting to be seen" metric doesn't always begin at the door. Originally, the "Door to MD / Mid-Level Treatment Begins" started when the patient first entered the door of the waiting area or the Emergency Trauma entrance of the Hospital.
The new metric doesn't start at the door. Now the starting point for this time measurement begins when the Registrar enters the patient's information into the computer, and that is generally when the patient is registered.
That happens after the patient has walked in the door, and after they have waited often at the end of a long line to speak to the registrar. Or simply waited for some time until a registrar or RN returned to the waiting area desk. Is this really the fair starting point for the patient's experience? No. The starting point is the moment they open the door and walk in or are rolled in.
A great deal of actual waiting time has been hidden from this highly touted new statistic, making it misleading.
But it makes the waiting time to RN, MD or Mid-level, indeed the entire Emergency Deparment Length of Stay look much better than it actually is!
Yes, metrics can be faked and often are.
These are all part of cutting corners on the metric to make the numbers look better because they are not actually part of making the flow more efficient for patients.
These times are not Door-to-MD / Mid-Level Treatment times according to the standardized, traditional metric.
DIRECT-TO-BED DONE WRONG MAKES THINGS WORSE
Some hospitals do bring patients directly to the bed in back when there is an empty and staffed bed, and this is a great strategy to reducing waiting time and potential medical error. But only so long as the RN completes the Triage work, initial labs, assessments and immediate interventions that are all part of the appropriate clinical pathway IMMEDIATELY when the patient is brought back. This expedites the MD /Mid-Level entering the room sooner to make their full assessment and begin formal intervention.
But Direct-to-Bed alone is not a fix and in isolation can make things worse, adding delay, neglect and medical error because, as we have seen, this can be used to warehouse a patient in the back where they are now isolated and still don't get rapid treatment.
Indeed, in some cases delays got longer, and clinical issues arose from those delays because the waiting room looked empty; the patient was now "out of sight - out of mind"; and no one really knew that the patient waiting in an Emergency Room bed in back hadn't yet been seen by RN, MD or Mid-level.
In fact, once they were placed into a bed in back, their actual status became a mystery - they fell into a crack in the process that looked on the tracking board like they were being assessed and treated, as though they had been seen by the RN but "seen" and "treated" are two different things - so the patient fell into a void, a twilight zone. On the tracking board, they were in a bed with an assigned nurse, maybe even seen by her or him so it looked like something was going on. But the RN assigned to that bed had not actually taken the assignment of that patient.
This is the problem with popular solutions that are not made in concert with actually changing the responsibilities, competencies, teamwork and communication points, but merely fixing the physical flow, or mechanically and mindlessly tracking data points in the computer.
Rather than fix the actual problems, some Hospitals have found a way to dissimulate (nice word for fibbing or misleading) by cutting corners on what they actually report as "waiting time". They compromise the original intention of waiting time: How long does the patient have to wait before their treatment begins? Door To Treatment!
In our discussion today, we aren't talking about the fake "Waiting Time in Our Emergency Department waiting Room" metric that some hospitals brag about and even post on bill boards and on the internet.
We are here talking about the real thing: The time from when the patient opens the door to enter the building to the time the MD or Mid-Level begins treatment.
And that time can be and is well under 30 minutes in the top performing hospitals - even in complex Trauma Centers that are also university teaching hospitals - such as Duke University Hospital - a shining example of this level of performance.
How can you take that next step in the journey of your own Emergency Department?
You can learn from the stuff we did with Duke and other Number One Hospitals:
We are here talking about the real thing: The time from when the patient opens the door to enter the building to the time the MD or Mid-Level begins treatment.
And that time can be and is well under 30 minutes in the top performing hospitals - even in complex Trauma Centers that are also university teaching hospitals - such as Duke University Hospital - a shining example of this level of performance.
How can you take that next step in the journey of your own Emergency Department?
You can learn from the stuff we did with Duke and other Number One Hospitals:
SEE THE FLOW - BE THE FLOW


 | ||
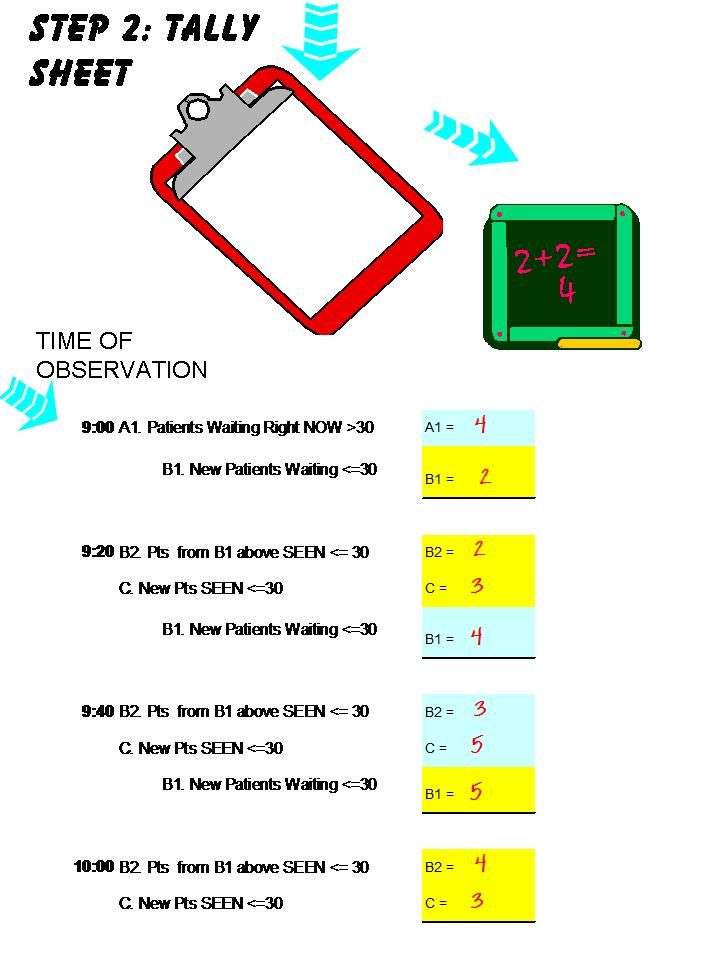
FIRST ROUND! Every twenty minutes the manager (yep, not the Charge at first, but the MANAGER or even the DIRECTOR - Hey, this is your home, right?) rounds through the waiting room and notes what is going on. Did I say this was permanent? No. Not every twenty minutes. One day it can be the Charge RN, when you see how valuable this is, how cost effective it is to give them the time to do this. But you are trying to make human behavioral change, so right now, it's every twenty minutes for a while, at least during the busy hours when waiting time is a problem. And it's the person with management authority and coaching skill to do it. No intermediaries, no layers, no committees. No excuses! This is the fastest way to make change - data, performance feedback and behavioral coaching and change all at once! So, it's worth the time. It's Kaizen, baby! Rapid Cycle PDCA many times a day! You'll get it on the way! A.1. When you go out for the first time and look around, you notice how many folks are in the waiting area, and you look at the log book / tracking report to see how many are waiting over 30 minutes. Maybe you talk with the Triage RN or the Registration Clerk. B1. And you also note the number of patients waiting 30 minutes or less. Now you go into the back, into the main ED and post your counts on the White Board for all to see, and make sure everyone you can grab sees these counts and talks with you about them. And each time you round, you come back and post your counts here on the white board, and you notice if things are getting worse or better, and try creating dialogue, interaction, connections, response and understanding: brainstorming on the fly, and innovation right there in your hands. And you are getting more control by asking questions, more effect by giving control to your team. But you won't know where the opportunities are to do this moment by moment unless you become the TRAFFIC QUEEN! (or King!). It's like hall monitor, you can assign the job to anyone, but first get the skills down. First, it's just positive reinforcement. How did the < 30 minute patients get moved through so quickly? Excellent! Find out now! Let them know you see it. Immediate Feedback! You've got Olympians there, in the rough! Great performance. This is what you can build upon, so get intimate with it first. See it, discuss it, understand why it works when it does. Did you even know you had these strengths in your team? If you did, then you haven't learned anything new! Keep looking! It isn't what you think. It can't be just what you think you know, otherwise you aren't seeing and learning. You will learn something new. Start by being open to it. It's power, it's a gold mine! That is what "the moment" really is. Your most powerful tool. Yet everyone knows there is more in the Moment than we can possibly fully understand. So people are afraid of it. It is dangerous to live there. And yet, avoiding it leads to errors, mistakes, poor care and service. And that is why an addiction to retrospective data is so destructive to managing in that moment, so eviscerating. And then, you can ask for suggestions around the waiting room times that take longer than 30 minutes. The first suggestions you will hear may be "We need to spend lots of money.....They - other department - need to do their jobs---." People may gravitate to the low personal threat answers- low personal change solutions - the ones that don't involve them very much. And therefore the ones almost impossible to make. The changes that you and your folks can make immediately are not always the ones that will be top of mind. People are looking at other people, not themselves. Or they cherry pick the few things that are truly out of their control. When you are there watching, listening, discussing, challenging, praising, questioning every twenty minutes, you will see that the opinions even just a day later are entirely tipped off balance and much less accurate. You will see that just seeing it NOW gives you accuracy you can't get any other way, and it also gives the communication with your staff ACCOUNTABILITY because they can't remember it in a more convenient way. The circumstances are there before you as physical evidence that has not passed into history, not dependent upon mere record. You can see the reality NOW while you can do something about it. And while the others around you can see it too, if you and they are willing to look and acknowledge. You will see that moment-by-moment decisions, habits, skills within the grasp of your own team significantly effect throughput, clinical errors, and the satisfaction of patients, their families, your MD partners, and your staff. Finally, you will see that you can cut delays in half by making course corrections on situations that have not yet fully completed: NOW is much more powerful than any sort of data analysis. And it is only in the NOW, in the department, on the floor, in the flow of work, that you can help others make permanent changes in vigilance, in ability to see and understand, in better behavior, and culture change. But these are not things that can be easily extrapolated by data. They are largely invisible without direct observation and real-time exploration. Data at best is an accurate shadow reflecting the outlines of what has happened but with little detail - it requires interpretation to understand. Reality in the NOW requires an open mind and willingness to observe, listen, inspect, dialogue. They are things you acknowledge directly because you see them, and things you show and state to others so they acknowledge them, too, instead of ignoring them. "Ignoring them": code words for ignoring patients. Praise may open the door, and gentle questions can open the door. Questions a day later are nearly useless, and much more threatening. Questions about the cause of a problem transform and magnify into implied blame after the fact, and typically result in defensive and less than candid responses. But in the moment, those inquiries can be put forth in the desire to help, to lend a hand while there is still time to do so. Questions about delays, acknowledging delays that are happening now can be greatly fixed now, while everyone is still there,while the process is still happening. And then the whole process was to build teamwork, was to share in the successful resolution and prevention of problems. Now you are handing that success to your team. What can be done now, with existing resources, with just a little creativity, coordination and teamwork? Just a little leadership in real-time can open up tremendous enthusiasm, creativity and growth. SECOND ROUND! And then you round back so that you are in the waiting area exactly 20 minutes from your first "count". This is where the wrist watch really helps! One with a repeating alarm is really great! Or an Android or iPhone Interval Trainer app can do that for you. B.2. How many patients that were waiting 30 minutes or less the last time are no longer in the waiting area because they have been admitted to the back? Great! C. How many patients are newly arrived since your last "count" and have already been admitted to the ED? Super Great! You won't see the C patients, but the time has been so short that the registration clerk, or the log or tracking sheet printout will show you. NEW B.1. How many patients are there that you haven't seen before but are now waiting? These are patients who have been waiting, so far, under 30 minutes. Now you go back to the white board and post your simple calculation, so everyone can see every twenty minutes during the busy hours, exactly how many patients are waiting, and how many of these are waiting over 30 minutes. HOW MANY PATIENTS ARE WAITING FOR MD > 30 MINUTES right NOW? OLD B.1. (B.1. from the prior round count) Minus B.2. = Patients who are now waiting > 30 minutes. HOW MANY PATIENTS HAVE BEEN SEEN AT OR UNDER 30 MINUTES DURING THE LAST 20 MINUTES? B.2. plus C. = Patients who have been seen at or under 30 minutes. It isn't just the fact that these numbers are posted in real-time that is so important. You are doing this, as a member of management, and discussing this, and trying to figure it out, and maybe fixing it in real-time. This sets up a whole new culture of accountability and safety, of self-control and empowerment: to state what is happening openly, respectfully; to ask to collaborate, ask questions, communicate a willingness to help, and a desire to act, with each other, without fear. How safe can a Hospital be for a patient if the RN doesn't think she or he has much control over things? That is an unsafe environment. And worse still when the MD thinks like that. But here you are practicing taking control by asking your own team to communicate with you as a team, to make decisions based on what they see right now, not to ignore it as out of control, but to take the extra step and make something good happen. What is very important is the fact that you are seeing exactly what is going on to create delay, and intervening where you can, coaching where you can, asking and helping where you can, right there. All of that flies in the face of the belief, the culture that says "it's out of our hands." It disproves the culture that says "only an expert.... only a committee....only a detailed analysis for months on end..... can fix this": all answers that push change farther and farther away. Unfortunately, that thinking pushes personal responsibility that far away, too. And that belief leads to choices every second of every day in the hospital: bad choices. At least 50% of most delays are not out of your hands. But to do something about it may mean suggesting something, asking something, directing and prioritizing. It's called being a good Traffic Cop. When you fix that 50% of the delay, you have power and leverage to go after the delay in other areas, since now there is no excuse for any manager to stay away from their daily operations. You are proving that a manager is only a leader when they do this. And no hospital, nor the patients in any department needs a manager who cannot lead. Many years ago many Emergency Departments had great traffic cops, many hospitals had great House Supervisors and Head Nurses, Senior Nuns who did just this sort of thing. They were the great ones. They were the masters of this art of dealing with the fully charged and infinite moment, effectively. This is an old practice. Very old. Largely lost. But no change can sustain, nor truly change patient's lives without mastering it. It requires a willingness to talk about it and ask for help, and step in and give the help as it is taking place, as reality is unfolding. But now folks just want to do it all on their own and in retrospect. Every employee is a silo. They want the world to be boiled down, filtered, photographed and manipulated into their laptop computer, into charts and reports that can be held in hand, put neatly into a folder, kept, used, leveraged. They want to live in a virtual world, which they can master and control. Every human being is isolated in this way to their own thoughts and the artificial virtual world in their own mind. But in Reality, in the Now, we are part of something bigger. We do not own this world. We participate. But we don't participate effectively if we ignore it, for any reason. So living in our own personal video game doesn't actually work in a Hospital. And life is better lived in this world, the real one, going forward. The only way to continue to look backward, at data, reports, in retrospect, to our own thoughts, to discussing what is already dead and gone, to dissecting what has no life in it is to turn one's back to the present and the future. Not a good idea. "Life can only be fully understood looking backward. But it must be lived moving forward." - Soren Kierkegaard TEAM or die! That's a literal truth in Hospitals! IN SUMMARY The first time you round you collect these points of data: A.1. and B.1. Every time you round after the first, you collect these three points of data: B.2. C. again and B.1. again And on your last round of the day, just collect these data points: B.2. and C. |
No comments:
Post a Comment